- My Forums
- Tiger Rant
- LSU Recruiting
- SEC Rant
- Saints Talk
- Pelicans Talk
- More Sports Board
- Fantasy Sports
- Golf Board
- Soccer Board
- O-T Lounge
- Tech Board
- Home/Garden Board
- Outdoor Board
- Health/Fitness Board
- Movie/TV Board
- Book Board
- Music Board
- Political Talk
- Money Talk
- Fark Board
- Gaming Board
- Travel Board
- Food/Drink Board
- Ticket Exchange
- TD Help Board
Customize My Forums- View All Forums
- Show Left Links
- Topic Sort Options
- Trending Topics
- Recent Topics
- Active Topics
Started By
Message
re: Testosterone-replacement therapy does not increase cardiac events in men
Posted on 9/13/23 at 1:24 pm to LEASTBAY
Posted on 9/13/23 at 1:24 pm to LEASTBAY
quote:
It's not the high libido likely causing divorce. I feel like it makes you talk back to your wife much easier.
I don’t know exactly what you’re getting at, but I do wonder about the psychological effects.
Feeling physically as I did in my twenties (better yet, how I could have felt if I had worked out then) sounds great, but acting/emoting/thinking etc as I did then does not appeal to me.
Doesn’t matter anyway, if it shuts down natural test production, I don’t see myself ever choosing it.
 2
2

Posted on 9/13/23 at 1:35 pm to tke_swamprat
quote:
I'm aware. I was replying to someone else just reporting another difference between the mode of treatment.
Yes, the difference between IM and other methods is well documented. Stan Effering has a good YouTube video about it. Maybe I did not word my point well. While not a direct heart correlation, IM DOES cause sides like increased HMG/HCT that can impact the heart, strokes, etc. How clinically significant that is is up for debate. I think Stan quotes 67% of IM users having this side vs. 16% of gel users. He goes on to say that there is a difference between erythrocytosis/increased RBC and polycythemia/blood thickening.

Posted on 9/13/23 at 1:39 pm to TigerAlum93
quote:
Yes, the difference between IM and other methods is well documented. Stan Effering has a good YouTube video about it. Maybe I did not word my point well. While not a direct heart correlation, IM DOES cause sides like increased HMG/HCT that can impact the heart, strokes, etc. How clinically significant that is is up for debate. I think Stan quotes 67% of IM users having this side vs. 16% of gel users. He goes on to say that there is a difference between erythrocytosis/increased RBC and polycythemia/blood thickening.
love stan but most people on trt never really get there hematocrit levels outside of normal range and if they do its not by much. if this was suck an issue than we would see people in high elevations falling out all the time. its not an issue.
you can also take Natt and essentially prevent any possibility of it
Posted on 9/13/23 at 1:43 pm to Earnest_P
quote:
wonder about the psychological effects.
there aren't psychological effects. You arent getting your levels supra-max
quote:
Feeling physically as I did in my twenties (better yet, how I could have felt if I had worked out then) sounds great, but acting/emoting/thinking etc as I did then does not appeal to me.
as mentioned you shouldnt be. for 1 you shouldnt have levels of a 18-21 year old at 40 even when on trt. You can if you choose but i personally think you should have upper ranges for your age. some like to say you should keep it to 1000 ng/dl and that is fine if you show no signs but i personally think it should be based on age for the most part
quote:
Doesn’t matter anyway, if it shuts down natural test production, I don’t see myself ever choosing it.
well you should only get on trt if you dont produce much naturally. Anytime you take an exogenesis hormone you are going to get a negative feedback loop that shuts down natural production. on trt this doesnt matter because you have made the decision to go on for a lifetime due to your body not producing much if at all naturally and certainly not for your age.
guess im confused on why you would care if natural production is shut down if you arent making much to begin with and are making the decision to go on for life
Posted on 9/13/23 at 1:54 pm to lsu777
quote:
guess im confused on why you would care if natural production is shut down if you arent making much to begin with and are making the decision to go on for life
Based on my own fairly naturalistic worldview, specifically that I think the natural reduction of test production with aging (beyond mid-life, especially) may be beneficial in allowing us to age well. “Age well” is up for interpretation but for me it includes growing in wisdom, the kind of wisdom that may only accrue with the reduction of testosterone. Also, not really wanting to look at pictures of naked chicks would be a feature of aging well.
This is all of course my own opinion, not judging others for wanting to feel younger and have more energy.
quote:
You can if you choose but i personally think you should have upper ranges for your age.
This balanced approach makes sense to me.
Posted on 9/13/23 at 2:00 pm to Earnest_P
quote:
Based on my own fairly naturalistic worldview, specifically that I think the natural reduction of test production with aging (beyond mid-life, especially) may be beneficial in allowing us to age well. “Age well” is up for interpretation but for me it includes growing in wisdom, the kind of wisdom that may only accrue with the reduction of testosterone. Also, not really wanting to look at pictures of naked chicks would be a feature of aging well.
yea frick all that
testosterone plays a big part in mental health btw and huge part of quality of life.
Posted on 9/13/23 at 2:09 pm to lsu777
quote:
Anytime you take an exogenesis hormone you are going to get a negative feedback loop that shuts down natural production.
What are the side effects of getting off TRT after let's say...a year?
Posted on 9/13/23 at 2:17 pm to gerberbaby22
quote:
What are the side effects of getting off TRT after let's say...a year?
you will need to do a full post cycle therapy and lets be clear going on trt for a year is just stupid. if you are going to shut down natural test, just do a cycle of 300-400mg min for 6 months.
atleast make it worth it. 120-150mg a week isnt going to give you any performance benefit unless you are already extremely low.
so side effects would be
- very low testosterone when you come off. you may be able to restart hpta axis and get back up to previous levels, maybe not.
- during the time you have the extreme low test you will have the symptoms of that
-it will effect sperm quality and quantity and you may not recover from this
its the same as coming off a steroid cycle
pct would need to be pretty inclusive
-2 different serms
- high doses of hcg
- if possible hmg
trt is a lifetime decision, coming on and off is not trt. What is your reason for asking?
This post was edited on 9/13/23 at 2:18 pm
Posted on 9/13/23 at 3:03 pm to lsu777
I'm 37, T level is 432, and Free T is 7.82. I've recently lost about 30 lbs, and have started lifting in the gym and riding mountain bike. I'm 194 lbs as of this morning.
I don't like that I'm so young and have seeming lowish T levels. Hoping that the gym work kick starts T levels, but some days I feel way lower and some days I feel more normal.
I only know what "normal" levels are based on what the doctor tells me and I'm not entirely convinced they're not trying to "sell" me. Are these levels low, and how long should I start seeing these numbers go up after starting to lift?
Today was the first day of doing squats and holy hell my legs/hamstrings are on fire.
I don't like that I'm so young and have seeming lowish T levels. Hoping that the gym work kick starts T levels, but some days I feel way lower and some days I feel more normal.
I only know what "normal" levels are based on what the doctor tells me and I'm not entirely convinced they're not trying to "sell" me. Are these levels low, and how long should I start seeing these numbers go up after starting to lift?
Today was the first day of doing squats and holy hell my legs/hamstrings are on fire.

Posted on 9/13/23 at 3:26 pm to lsu777
quote:
yea frick all that
100% agree with you 777!
I feel great on it. My wife gets annoyed at times, but she goes with the flow.

Posted on 9/13/23 at 3:35 pm to WhiskeyThrottle
quote:
Today was the first day of doing squats and holy hell my legs/hamstrings are on fire.
Just wait until to have to sit down to shite tomorrow.
Posted on 9/13/23 at 4:18 pm to lsu777
quote:
well here is a study saying its not
FIFY
Posted on 9/13/23 at 9:11 pm to lsu777
Wish my doctor would read this board. Dude says 350 is a perfectly fine level, and this aint an OT joke.
Posted on 9/13/23 at 9:31 pm to BadatBourre
Find a new doctor is best answer I can give you.

Posted on 9/13/23 at 9:32 pm to Earnest_P
quote:
I don’t know exactly what you’re getting at, but I do wonder about the psychological effects.
It changed my personality a bit. For the better mostly though. I just didn't put up with as much shite from people once I started it. Been on trt about 3 years now.
Posted on 9/14/23 at 5:53 am to BadatBourre
quote:
Wish my doctor would read this board. Dude says 350 is a perfectly fine level, and this aint an OT joke.
You aren't the only one. I pay $300 a month at a clinic for test plus hcg. It is fricking insanely expensive and I really do not want to pay it. The amount of help it has been for the past 3-4 weeks though has been profound. I may have found a doctor, but no idea how she will react. I'm on my 3rd doctor...no one wants to help when my range was 311-330.
Posted on 9/14/23 at 6:28 am to lsu777
This is a topic that gets my pisstivity levels sky high. Been trying to educate people about this topic for a long time. You'd be amazed at the number of clinicians who were told long ago about negative effects, have never looked at literature since their training, and go on to teach others the same thing.
There was a paper that came out in 2013 in JAMA that did immense damage to TRT. Lead author Vigen. It's the worst and most irresponsible statistical analysis I've ever seen in such a contentious subject. Claimed increased cardiovascular risk. I think it's very likely the true result was in the opposite direction. Paper should have been retracted but journals never want to go down that road.
They used stabilized weights in an extended Kaplan Meier survival analysis, and with messy data the test statistic behaves in a wildly erratic manner. This always produces messy data. Simulations have demonstrated this. Not only this, but they had a very high amount of misclassification, which plays into the messy data.
I mean this honestly, I think I know more about that analysis than anyone else in the world. It's just awful. Additionally, the data generating mechanism is a change state model, which is intractable mathematically. They tried Kaplan Meier but that was the wrong choice, then used stabilized weights which was insane - the whole thing was a disaster - yet the FDA cited it prominently in its decision to issue a warning about TRT.
I worked in research at the VA and published on this topic. I also looked at VA data and found that as time went on, people were spending more and more time off of their TRT, when looking at their prescription data, so compliance was spotty at best and had significant gaps between prescriptions when their levels were clearly going to be very low.
I tried to draw attention to this while working at the VA - I got the data, did the analysis, pointed out some flaws with Vigen and other papers, and called for a re-look at a lot of TRT data and a better understanding of the stats being used, the nature of TRT usage etc. Very simple paper. Contacted Annals of Internal Medicine (very prestigious journal) and asked for expedited review due to the nature of this topic, they agreed. Got rejected because they thought the paper was sloppy because citation information wasn't complete for a couple references. It wasn't complete because when the paper was written the citation information had not been completed by the publisher - these studies were brand new and journals put them on PubMed without knowing which volume and page they would end up on. By the time the papers got to a reviewer that info had been updated and the reviewers didn't bother to connect the dots on this. I'm still chapped about this.
The statistical analysis for these types of papers is very sophisticated and there are too many people winging it just because the computing power is available. I contacted another journal a guy had just started, devoted specifically to these analytical issues. I asked the editor if he was interested and he said yes. One of the journal editors was part of the team that put out one of the modeling procedures for these types of analyses and I specifically wanted his commentary. I also met with a lady at UF who was part of that team - she was unbelievably rude and dismissive. Harvard person. That journal required a certain software be used for manuscript generation. I put in a request with the VA to have installed on my computer - the funding for my position expired before I ever heard from the VA, so that never happened.
There was heavily flawed research in the early days about testosterone and it got the bad rep of being related to prostate cancer and CVD. If you go to PubMed and look for an author, Morgentaler, lot of free articles you can get with him - he has written about this, the history etc.
Injection produces an early peak then a gradual decline in levels. Pretty potent stimulator of blood cell production, which is why doctors like to look at things like hematocrit when you're on TRT. Transdermal (gel) TRT isn't as pronounced at blood cell production, but the enzyme that converts T to DHT is present in higher amounts in the skin so you will get more conversion to DHT, which has aroused some debate over the years. Transdermal is not going to produce the peaks and valleys like injection, but it's daily, not weekly or bi-weekly.
This graph is pretty good. Note with injection on a typical schedule, that the person will be back to baseline and a low T level for some time prior to another injection, and right after the injection a person can zoom into supraphysiological levels. Gel presents its own problems though, like needing to avoid skin to skin contact, more DHT production etc.
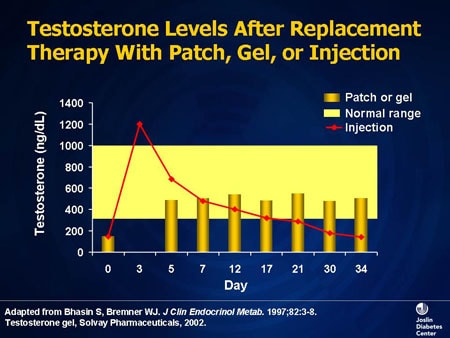
There are some differences between the two routes, but not like night & day such that your entire outlook or physiological profile will change.
Injection may be safer
Elevation of DHT and CV risks vary by route
T deficiency historical perspective
Edit - on that graph, the same phenomena is seen whether your injections are weekly, bi weekly, monthly etc. Typically you see 100mg/wk or 200mg/bi-weekly and so forth. Data I've seen is overwhelmingly a 200mg/bi-weekly approach. Generally what you see is this: shorter injection interval means less time back at/below baseline prior to next injection and less of a peak, while longer interval will be a larger peak and longer number of days at/below baseline prior to the next injection. Holy grail might be oral TRT, but prior formulations were toxic to the liver, but I believe they are still working on this. One of the uses for T is male contraception, but even when they've given guys 250mg/wk they still see some residual sperm production, so I don't think they've cracked the code on that - it's noteworthy that in such studies they rarely saw deleterious effects such that guys discontinued.
Also, for the people you encounter that think TRT is so much of a risk, I always point out that epidemiological studies of older eastern bloc athletes that were on the juice, showed no health effects and that we never see alarming levels of prostate cancer in powerlifters, strong men and others that we know to be on high doses, chronically. And in old school bodybuilders, they were not pitching clots and dying young like we see today, where guys are on a huge cocktail of stuff at insane levels.
Lastly, in a large VA study of prostate cancer where they blocked T production, within six months guys had severe health problems from depression to diabetes to occult cardiovascular disease. Adequate T is absolutely essential for men.
There was a paper that came out in 2013 in JAMA that did immense damage to TRT. Lead author Vigen. It's the worst and most irresponsible statistical analysis I've ever seen in such a contentious subject. Claimed increased cardiovascular risk. I think it's very likely the true result was in the opposite direction. Paper should have been retracted but journals never want to go down that road.
They used stabilized weights in an extended Kaplan Meier survival analysis, and with messy data the test statistic behaves in a wildly erratic manner. This always produces messy data. Simulations have demonstrated this. Not only this, but they had a very high amount of misclassification, which plays into the messy data.
I mean this honestly, I think I know more about that analysis than anyone else in the world. It's just awful. Additionally, the data generating mechanism is a change state model, which is intractable mathematically. They tried Kaplan Meier but that was the wrong choice, then used stabilized weights which was insane - the whole thing was a disaster - yet the FDA cited it prominently in its decision to issue a warning about TRT.
I worked in research at the VA and published on this topic. I also looked at VA data and found that as time went on, people were spending more and more time off of their TRT, when looking at their prescription data, so compliance was spotty at best and had significant gaps between prescriptions when their levels were clearly going to be very low.
I tried to draw attention to this while working at the VA - I got the data, did the analysis, pointed out some flaws with Vigen and other papers, and called for a re-look at a lot of TRT data and a better understanding of the stats being used, the nature of TRT usage etc. Very simple paper. Contacted Annals of Internal Medicine (very prestigious journal) and asked for expedited review due to the nature of this topic, they agreed. Got rejected because they thought the paper was sloppy because citation information wasn't complete for a couple references. It wasn't complete because when the paper was written the citation information had not been completed by the publisher - these studies were brand new and journals put them on PubMed without knowing which volume and page they would end up on. By the time the papers got to a reviewer that info had been updated and the reviewers didn't bother to connect the dots on this. I'm still chapped about this.
The statistical analysis for these types of papers is very sophisticated and there are too many people winging it just because the computing power is available. I contacted another journal a guy had just started, devoted specifically to these analytical issues. I asked the editor if he was interested and he said yes. One of the journal editors was part of the team that put out one of the modeling procedures for these types of analyses and I specifically wanted his commentary. I also met with a lady at UF who was part of that team - she was unbelievably rude and dismissive. Harvard person. That journal required a certain software be used for manuscript generation. I put in a request with the VA to have installed on my computer - the funding for my position expired before I ever heard from the VA, so that never happened.
There was heavily flawed research in the early days about testosterone and it got the bad rep of being related to prostate cancer and CVD. If you go to PubMed and look for an author, Morgentaler, lot of free articles you can get with him - he has written about this, the history etc.
Injection produces an early peak then a gradual decline in levels. Pretty potent stimulator of blood cell production, which is why doctors like to look at things like hematocrit when you're on TRT. Transdermal (gel) TRT isn't as pronounced at blood cell production, but the enzyme that converts T to DHT is present in higher amounts in the skin so you will get more conversion to DHT, which has aroused some debate over the years. Transdermal is not going to produce the peaks and valleys like injection, but it's daily, not weekly or bi-weekly.
This graph is pretty good. Note with injection on a typical schedule, that the person will be back to baseline and a low T level for some time prior to another injection, and right after the injection a person can zoom into supraphysiological levels. Gel presents its own problems though, like needing to avoid skin to skin contact, more DHT production etc.
There are some differences between the two routes, but not like night & day such that your entire outlook or physiological profile will change.
Injection may be safer
Elevation of DHT and CV risks vary by route
T deficiency historical perspective
Edit - on that graph, the same phenomena is seen whether your injections are weekly, bi weekly, monthly etc. Typically you see 100mg/wk or 200mg/bi-weekly and so forth. Data I've seen is overwhelmingly a 200mg/bi-weekly approach. Generally what you see is this: shorter injection interval means less time back at/below baseline prior to next injection and less of a peak, while longer interval will be a larger peak and longer number of days at/below baseline prior to the next injection. Holy grail might be oral TRT, but prior formulations were toxic to the liver, but I believe they are still working on this. One of the uses for T is male contraception, but even when they've given guys 250mg/wk they still see some residual sperm production, so I don't think they've cracked the code on that - it's noteworthy that in such studies they rarely saw deleterious effects such that guys discontinued.
Also, for the people you encounter that think TRT is so much of a risk, I always point out that epidemiological studies of older eastern bloc athletes that were on the juice, showed no health effects and that we never see alarming levels of prostate cancer in powerlifters, strong men and others that we know to be on high doses, chronically. And in old school bodybuilders, they were not pitching clots and dying young like we see today, where guys are on a huge cocktail of stuff at insane levels.
Lastly, in a large VA study of prostate cancer where they blocked T production, within six months guys had severe health problems from depression to diabetes to occult cardiovascular disease. Adequate T is absolutely essential for men.
This post was edited on 9/14/23 at 6:40 am
Posted on 9/14/23 at 6:52 am to BadatBourre
If you’re going to your PCP for TRT, you’ll have a hell of a time because they typically only treat if your levels are actually below normal on 2 separate blood draws done before 10am. This is an insurance thing.
The best bet is to go to a wellness clinic where you’re more than likely going to see a NP who is going to treat your symptoms and not just the number. Most don’t take insurance so it’s out of pocket. But realistically a bottle of test is cheap with GoodRx, so it all depends amhow much they charge for the visit and lab work.
The best bet is to go to a wellness clinic where you’re more than likely going to see a NP who is going to treat your symptoms and not just the number. Most don’t take insurance so it’s out of pocket. But realistically a bottle of test is cheap with GoodRx, so it all depends amhow much they charge for the visit and lab work.

Posted on 9/14/23 at 7:17 am to Junky
quote:
You aren't the only one. I pay $300 a month at a clinic for test plus hcg. It is fricking insanely expensive and I really do not want to pay it. The amount of help it has been for the past 3-4 weeks though has been profound. I may have found a doctor, but no idea how she will react. I'm on my 3rd doctor...no one wants to help when my range was 311-330.
Where are you located?
My doc checks my labs once per year. It's about $100 for that visit then he does a 6 month video checkup before renewing my prescription, that's my copay. Test would be $80 a vial from Amazon pharmacy but insurance covers it. It's $10 every 14 weeks. Even if I didn't have insurance I'd be wayyyyy under the $300 a month. I was a little lower than you but not much.
Posted on 9/14/23 at 7:45 am to POTUS2024
quote:
POTUS2024
first off HOLY shite!! great post
quote:
on that graph
everyone can you steroidcalculator.com and plot out the graph. a twice weekly injection will have you around baseline around day ~30. Lets say you would take the standard dose of 150mg 2x weekly(essentially every 3.5 days) and going IM. Assuming cypionate ester you would reach absolute peak serum levels at day 35 but would be pretty damn close to peak after only 3 weeks. Levels would bounce between ~12mg to little over 18mg~ released in the blood. That is pretty damn stable levels and would represent essentially zero risk on health.
I will say on the gel...outside of the risk of transmission(huge for those with kids) and dht levels, the other issue is maintaining consistent blood levels is much harder due to the nature of transdermals themselves.
biggest issue is the absorption rate. Even with a molecular weight under 350 which is around the highest you can consistently pull through the skin....you still have at max a 20-25% conversion (testosterone no ester is ~288g/mol). That is best case. But absorption is dependent on you have taken a shower, scrubbed really hard to get all old dead skin off, making sure the area stays perfectly hydrated, that the area has high absorption rate capability etc etc
in the end with the gel you end up with levels all over the map because there are so many variables.
quote:
POTUS2024
can i ask how you feel about the study from Cal on the use of Subq vs IM? LINK that is the power point on it. dont have the actual study, maybe you can find.
they found
14% greater Total t in subq vs IM
41% lower avg hematocrit subq vs IM
26.5% lower estrodiol
no rise in PSA
i think this is the study LINK

 Page 2 of 4
Page 2 of 4

Popular
Back to top