- My Forums
- Tiger Rant
- LSU Recruiting
- SEC Rant
- Saints Talk
- Pelicans Talk
- More Sports Board
- Fantasy Sports
- Golf Board
- Soccer Board
- O-T Lounge
- Tech Board
- Home/Garden Board
- Outdoor Board
- Health/Fitness Board
- Movie/TV Board
- Book Board
- Music Board
- Political Talk
- Money Talk
- Fark Board
- Gaming Board
- Travel Board
- Food/Drink Board
- Ticket Exchange
- TD Help Board
Customize My Forums- View All Forums
- Show Left Links
- Topic Sort Options
- Trending Topics
- Recent Topics
- Active Topics
Started By
Message
re: Coronavirus Disease 2019 (COVID-19) ***W.H.O. DECLARES A GLOBAL PANDEMIC***
Posted on 5/28/20 at 8:45 am to Tiguar

Posted on 5/28/20 at 8:45 am to Tiguar
quote:
I highly suspect history is going to judge the left and media harshly for downplaying HCQ.
They certainly need to be held accountable if there is strong evidence it works in early treatment.
 0
0

Posted on 5/28/20 at 9:05 am to buckeye_vol
quote:
I just don’t know how they arrived at this estimate. The meta-analysis of IFR estimates is now up to 25 IFR studies worldwide, and they now estimate the IFR at 0.64% (0.71% average across all 25) and the lower bound estimate of all 25 (95% CI) is 0.5%. Only 4 of the 25 are below 0.35%.
I was under the assumption that the lower IFR was only applicable to infections occurring now (i.e. after a few months of getting the medical side down a little bit). I don't know if they're taking say, a 40% reduction due to improved treatment (less use of ventilators, at least an agreed upon treatment protocol, etc...)
It would be a misuse to apply to past infections or use it to reverse calculate the number of people infected to date (although I don't doubt some of the folks on this board are going to attempt just that).
I don't know if I agree with WaWa's theory that they're taking into account demographics and assuming that we've reached saturation in the nursing homes. In the Northeast and Louisiana maybe, but I don't know if we can say the same thing about population heavy hitters (TX, CA, OH)
I also think it may be higher because younger people just flat out aren't getting infected - and there aren't enough middle aged folks to offset the elderly.
Posted on 5/28/20 at 9:23 am to Tiguar
The media didn't really downplay HCQ, they attacked it with full force from the moment Trump mentioned it and well before there was any strong evidence one way or another. They even started by attacking the safety profile of one of the most studied and administered drugs ever. They suggested we couldn't use it for a pandemic because that might deprive lupus and RA patients of the drug. And then they seized on a series of inconclusive or just plain bad studies in their fervor to discredit and discourage it's use. I've never read so many wildly inaccurate, one-sided, and blatantly biased viewpoints on a medication in my life, including some from publications in the healthcare media spectrum.
Amazingly, we still don't have any good data to say if the drug works well enough to make a significant difference in early or prophylactic Covid use, even though it's seen heavy outpatient use since mid to late March in places like Italy. Unfortunately, when we start seeing political opinions permeate medical journals, I'm not sure if HCQ can be depoliticized enough to ever get a reasonable answer; a long history of brutal interaction between dogma and science says maybe not.
Amazingly, we still don't have any good data to say if the drug works well enough to make a significant difference in early or prophylactic Covid use, even though it's seen heavy outpatient use since mid to late March in places like Italy. Unfortunately, when we start seeing political opinions permeate medical journals, I'm not sure if HCQ can be depoliticized enough to ever get a reasonable answer; a long history of brutal interaction between dogma and science says maybe not.
This post was edited on 5/28/20 at 10:21 am
Posted on 5/28/20 at 11:19 am to WaWaWeeWa
quote:
We found that the small vessels and capillaries in the lungs were obstructed by blood clots and associated hemorrhage that significantly contributed to decompensation and death in these patients
It sounds like a limited form of DIC.
Edit: while looking around to see more about this, I found these two articles about lupus anticoagulants, which are anti-phosphlipid antibodies. Unclear if LAC represent correlation or causation of thrombosis (2nd article suggests causation, at least in SLE), but I thought it was interesting anyway.
Lupus Anticoagulant in COVID-19: Culprit or correlate?
quote:
•Lupus anticoagulant isn’t any single thing, but instead it refers to a variety of different antibodies which may behave differently in different patients. The defining feature of these antibodies is that they bind to phospholipids, causing interference in in vitro clotting tests that require phospholipid (most notoriously the aPTT).
•However, in vivo, these antibodies are often associated with hypercoagulability (via mechanisms which are poorly understood).
•So yeah – lupus anticoagulant makes the coagulation labs look like the patient is bleedy, but in reality the patient may be clotty.
quote:
•Lupus anticoagulant is present in lots of COVID-19 patients if it is carefully sought after using dedicated tests, such as the Russell viper venom assay and modified aPTT (perhaps roughly 50-75%, depending on disease severity).
•Fewer COVID-19 patients have a prolonged aPTT level using standard assays (perhaps ~20%). Among these patients, the great majority (~90%) might have lupus anticoagulant.
quote:
lupus anticoagulant can rarely be found in asymptomatic people.
•Viral infections can often cause a transient, infrequent production of lupus anticoagulant. This is of unclear significance, but in some situations these have been correlated with increased risk of thrombosis.?3?
•Lupus anticoagulant can occur transiently in the context of patients with acute thrombosis. It’s not entirely clear what role exactly the lupus anticoagulant might be playing here.
•Persistent presence of lupus anticoagulant for >12 weeks combined with evidence of thrombosis may satisfy diagnostic criteria for antiphospholipid antibody syndrome. This is a pro-thrombotic condition which requires therapeutic anticoagulation.
This one is from 2013 Journal of Rheumatology
Hydroxychloroquine Use is Associated with Lower Odds of Persistently Positive Antiphospholipid Antibodies and/or Lupus Anticoagulant in SLE
quote:
Antiphospholipid antibodies (aPL Abs) play an active role in the pathogenesis of the antiphospholipid syndrome (APLS). Primary prevention in APLS may be aimed at decreasing existing elevated aPL Ab levels, or preventing high aPL titers and/or lupus anticoagulant (LAC) from developing in the first place.
quote:
Hydroxychloroquine (HCQ) has been shown to decrease aPL titers in laboratory studies, and to decrease thrombosis risk in systemic lupus erythematosus (SLE) patients in retrospective studies. We investigated an association between HCQ use and persistent aPL Abs and/or LAC in SLE.
quote:
Results: Among 90 patients included in the study, 17 (19%) had persistent LAC+ and/or at least one aPL Ab = 40 units. HCQ use was associated with significantly lower odds of having persistent LAC+ and/or aPL Abs = 40 U, OR 0.21 (95% CI 0.05, 0.79) p=0.02, adjusted for age, ethnicity, and gender.
quote:
HCQ treatment is currently recommended for SLE patients with persistent moderate-high aPL Ab or LAC+ for primary prevention (grade 1B to 2B recommendation) based on the other beneficial effects of HCQ in SLE (12, 13) and thrombosis (14). However, this is the first study to show that HCQ use may be associated with lower odds of having persistently positive LAC and/or aPL Abs in SLE, and, therefore, may be beneficial in primary prevention.
This post was edited on 5/28/20 at 12:05 pm
Posted on 5/28/20 at 12:48 pm to WaWaWeeWa
quote:Ummm that’s for a very specific reason: base rates. When base rates are low, specificity is the bigger concern as the positive predictive value is lower. But as base rates rise then sensitivity becomes more of a concern and the negative predictive value lowers.
As soon as there is an antibody study you just harp on the false positive problem without even giving any time to the possibility that the antibody studies aren’t detecting every patient who has encountered this virus.
quote:I am consider this, which is why I’ve been focusing so much on the NYC data because their deaths skew YOUNGER (as it is a younger and healthier city than than the US overall) than the flu plus they have detailed demographic data AND their base rates are highest in the country (if not world).
You aren’t considering the fact that nursing homes and long term care facilities have been hit way harder than the general population.
Anyways, as an example, in 2017-2018, the deadliest flu season in decades with 61,099 deaths and a a 0.14% symptomatic case fatality rate, 83.3% of the deaths were from those 65 and older (80% is about average anyways). Currently in NYC, 74% of the deaths are from those 65 and older.
In other words, while it is still much deadlier the older one gets, in NYC at least, it’s actually skewing younger than the FLU, and that’s with fewer infections among the youngest population (compared to FLU at least, regardless of the reason).
And they’re looking at an IFR around 0.8% to 1% based on the antibody data (which is more reliable because of the base rates although I would like more details and some follow-up prevalence data).
quote:BECAUSE THEY DIDN’T PROVIDE ANY SUPPORTING DATA OR DOCUMENTATION.
I’m not surprised at all that you can’t figure out how they arrived at that number.
And apparently I’m not the only one. And note while this is a Buzzfeed article, it was a Nation Review writer (conservative publication) who cited it because he was confused about the basis as well.
The CDC Released New Death Rate Estimates For The Coronavirus. Many Scientists Say They’re Too Low.
quote:That bolder portion is the strangest part to me. Why are CDC estimates based on a study from Iranian scientists?
Researchers also lambasted the CDC’s lack of transparency about its data sources. The eight-page document disclosed almost nothing about its numbers, citing only internal data and a preprint — a study that has not been peer-reviewed — led by scientists in Iran.
This post was edited on 5/28/20 at 12:59 pm
Posted on 5/28/20 at 1:42 pm to buckeye_vol
quote:
Ummm that’s for a very specific reason: base rates. When base rates are low, specificity is the bigger concern as the positive predictive value is lower. But as base rates rise then sensitivity becomes more of a concern and the negative predictive value lowers.
My point is you don’t even know what the definition of immunity is. Is the only person who is immune or who has beaten the disease show antibodies? There is mounting evidence that’s not entirely true.
quote:
I am consider this, which is why I’ve been focusing so much on the NYC data because their deaths skew YOUNGER (as it is a younger and healthier city than than the US overall) than the flu plus they have detailed demographic data AND their base rates are highest in the country (if not world).
They seeded all their most vulnerable High density populations (nursing homes) with 4,200 infected patients, and there are a lot of questions regarding their classification of deaths and “suspected deaths”
quote:
That bolder portion is the strangest part to me. Why are CDC estimates based on a study from Iranian scientists?
The cited internal data. I trust they have facts that we don’t.
I’m 100% positive that if the cdc came out and said the IFR was 1% you would be saying that is the absolute truth. Instead they didn’t say what you wanted them to so you are looking for reasons to discredit them.

Posted on 5/28/20 at 1:50 pm to Ronaldo Burgundiaz
Re: Efficacy of lockdowns/shelter-in-place
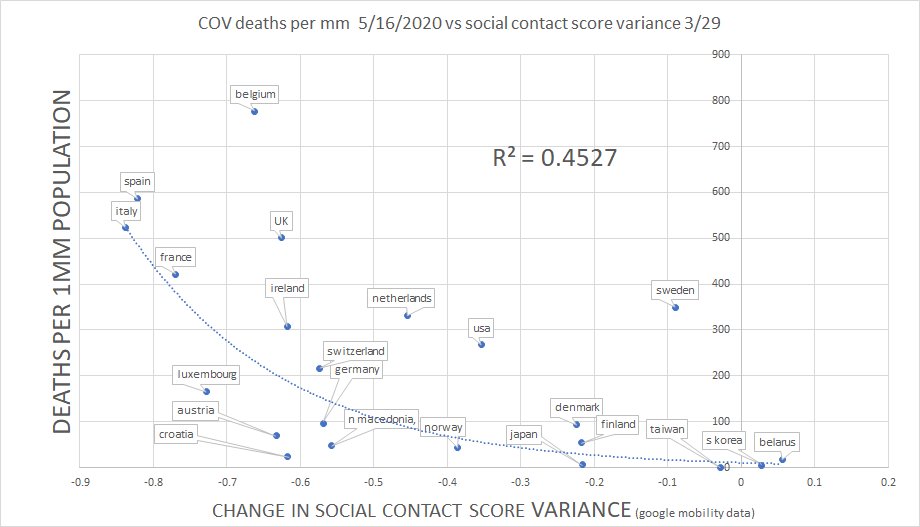
A really, really solid read here with a lot of charts and graphs: https://threadreaderapp.com/thread/1261705308302270466.html
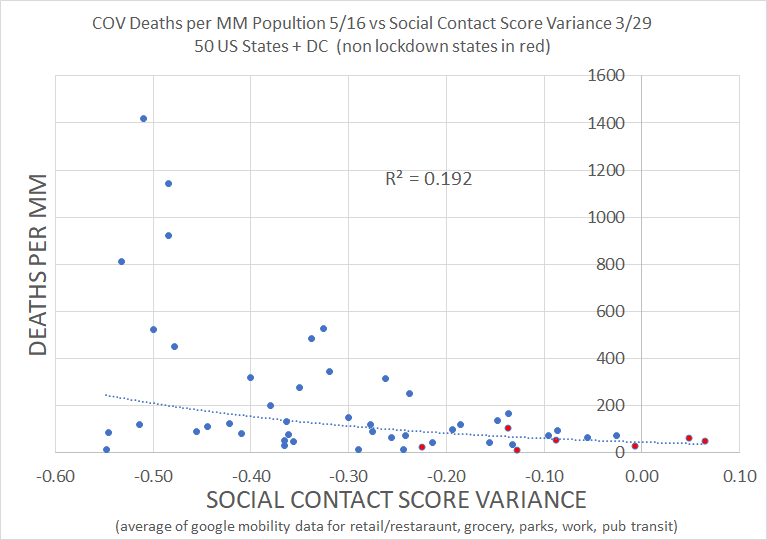
Twitter baw compares deaths per million data against Google's mobility score change and finds no correlation between the change in mobility and lower deaths per million, in fact, its inverse:
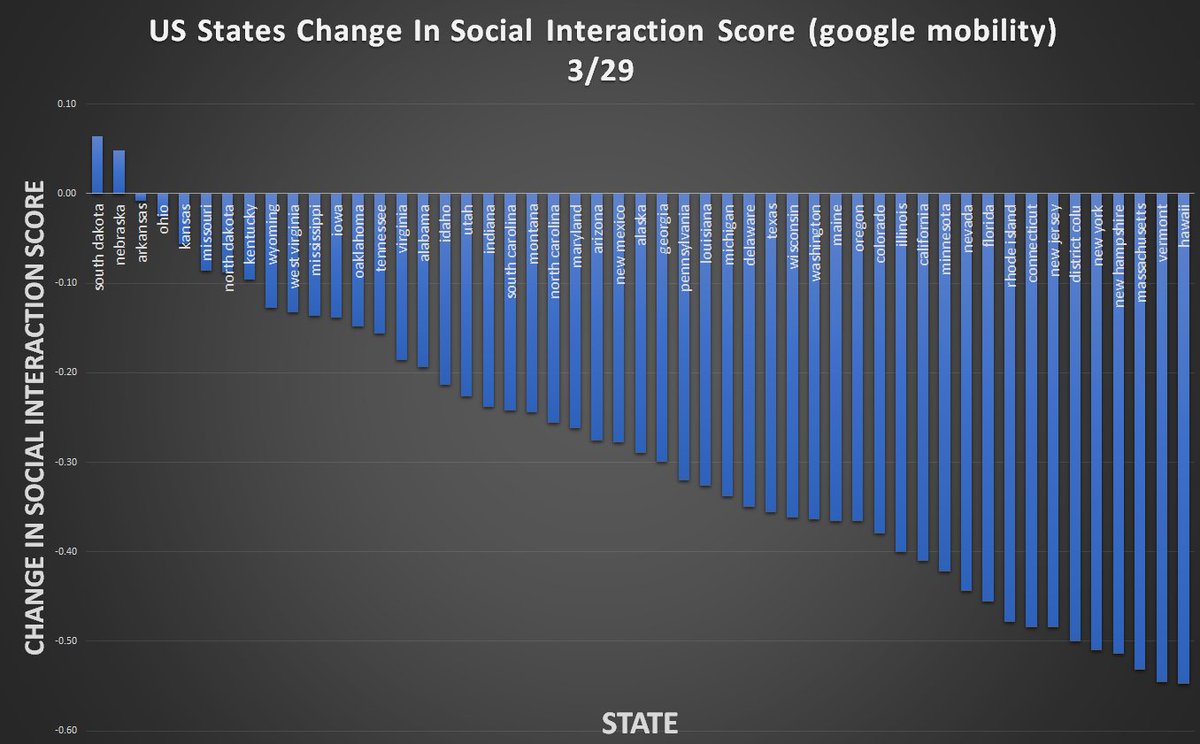
US state mobility score change:
He also points out that the CDC's own guidelines point out that once a virus hits 1% prevalence lockdowns are useless (remember, scientists pointed out that the virus had been circulating in Seattle for around 6 weeks before the first death was recorded:

Even if we locked down in January and prevented this. What then? We would have to continue locking down until the rest of the world had its course of covid ran through. Example: we beat it back in January with lockdowns, an asymptomatic carrier flies in Brazil today and super spreads it in the airport. Guess what we have to start all over.
It really seems like the driving factor in deaths per million is the nursing home/LTC policies of the governments, not so much lockdown/shelter-in-place.
A really, really solid read here with a lot of charts and graphs: https://threadreaderapp.com/thread/1261705308302270466.html
Twitter baw compares deaths per million data against Google's mobility score change and finds no correlation between the change in mobility and lower deaths per million, in fact, its inverse:
US state mobility score change:
He also points out that the CDC's own guidelines point out that once a virus hits 1% prevalence lockdowns are useless (remember, scientists pointed out that the virus had been circulating in Seattle for around 6 weeks before the first death was recorded:
Even if we locked down in January and prevented this. What then? We would have to continue locking down until the rest of the world had its course of covid ran through. Example: we beat it back in January with lockdowns, an asymptomatic carrier flies in Brazil today and super spreads it in the airport. Guess what we have to start all over.
It really seems like the driving factor in deaths per million is the nursing home/LTC policies of the governments, not so much lockdown/shelter-in-place.
Posted on 5/28/20 at 2:08 pm to WaWaWeeWa
quote:What?
My point is you don’t even know what the definition of immunity is.
quote:I don’t know. Like Matt Damon in the movie Contagion (which is supposed to be pretty scientifically accurate), I wouldn’t at all he surprised that there are some people who are completely immune despite never having the virus.
Is the only person who is immune or who has beaten the disease show antibodies?
quote:And I’ve even ACKNOWLEDGED TO YOU in another thread that I believe this is entirely possible.
There is mounting evidence that’s not entirely true.
But while that could have a major impact on the population level immunity (specifically to get to her immunity) and thus the overall mortality that has less to do with the IFR discussion regarding people who did not have that innate immunity.
quote:Well then. Since you say this:
They seeded all their most vulnerable High density populations (nursing homes) with 4,200 infected patients, and there are a lot of questions regarding their classification of deaths and “suspected deaths”
quote:Then you should be relieved based in this WSJ article from today that cites the CDC:
The cited internal data. I trust they have facts that we don’t.
Most Countries Fail to Capture Extent of Covid-19 Deaths
quote:
”We’re almost sure there’s undercounting, not overcounting” in the U.S., said Robert Anderson, chief of the mortality statistics branch at the CDC’s National Center for Health Statistics.
quote:I cited a meta-analysis that put the IFR between 0.5% and 0.8% to justify my concerns with the CDC estimates. You know what I didn’t cite: a University of Washington estimate of symptomatic CFR (i.e., comparable to CDC’s 0.4%) of 1.3% and a Stanford University study (from the department of biology) that estimated the global IFR at 1.04%, both of which were released in the past couple of weeks. Although I would include them (like the Santa Clara study I’ve been so critical of) with the rest of the studies in the meta-analysis (if they meet the inclusion guidelines).
I’m 100% positive that if the cdc came out and said the IFR was 1% you would be saying that is the absolute truth. I
I based my views off of dozens of studies, instead of just 1 that fit my priors. In fact, I previously thought (before we had data) it would be around 1%, and I’ve adjusted downward as the multiple data sources suggest it’s lower.
So clearly you’re wrong since I could have used a single source that supported the 1% but chose to use multiple sources that support a lower IFR.
This post was edited on 5/28/20 at 2:11 pm
Posted on 5/28/20 at 2:19 pm to buckeye_vol
quote:
What?
I’m saying no one knows what the definition of immunity is or how to accurately define who has been infected.
Just last night I posted a study that showed healthcare works with no detectable antibodies in their blood but antibodies in the mucous membranes. Are people like that counted in your Meta-analysis?
quote:
So clearly you’re wrong since I could have used a single source that supported the 1% but chose to use multiple sources that support a lower IFR.
I’m going to go with the CDC on this one. When someone goes against what you would expect, there usually is a good reason.
I would fully expect the CDC to err on the side of caution and to continue to oversell the pandemic so people practice caution. They went completely against that. If they are acting nefariously then you would have to give me a good reason why.
Posted on 5/28/20 at 2:23 pm to buckeye_vol
quote:
You know what I didn’t cite: a University of Washington estimate of symptomatic CFR (i.e., comparable to CDC’s 0.4%) of 1.3% and a Stanford University study (from the department of biology) that estimated the global IFR at 1.04%, both of which were released in the past couple of weeks.
Did you put as much effort into critiquing those studies to show why they were wrong in their conclusions as you do for the studies that show a low number?
Posted on 5/28/20 at 2:32 pm to Sasquatch Smash
quote:Since I barley saw any discussions about them, let alone people touting them as proof positives of the true IFR, I didn’t even pay much attention to them since they were just 2 of dozens of estimates that would only marginal impact the aggregate estimation, just like the Santa Clara study on the opposite side of the distribution.
Did you put as much effort into critiquing those studies to show why they were wrong in their conclusions as you do for the studies that show a low number?
And just like the Santa Clara study, I think that each study has its strengths, weaknesses, biases, etc., and no single study should be considered the “correct” one, which is why meta-analyses are so important to science (particularly social sciences) and usually provide a more reasonable and accurate estimation of whatever phenomenon (wisdom of the crowd sort of thing).
Posted on 5/28/20 at 2:37 pm to buckeye_vol
quote:
Since I barley saw any discussions about them, let alone people touting them as proof positives of the true IFR, I didn’t even pay much attention to them
Well, you could have brought them here to discuss them with the group.
Posted on 5/28/20 at 2:38 pm to buckeye_vol
Meta-analysis is completely irrelevant if the metric they are using to determine an infection is wrong
Posted on 5/28/20 at 2:45 pm to WaWaWeeWa
quote:1. Point out what is wrong then.
Meta-analysis is completely irrelevant if the metric they are using to determine an infection is wrong
2. Point out what is RIGHT OR WRONG with the CDC estimates and how they came to those conclusions.
I’m not saying the CDC IS WRONG, but I’m saying that they didn’t provide what is necessary to make ANY DETERMINATION, especially because the vast majority of studies that have do not support those estimates.
Is it to much to expect them to show their work, especially since multiple organizations (both right and left) and scientists have requested it and gotten NO RESPONSE.
Posted on 5/28/20 at 3:43 pm to Ronaldo Burgundiaz
Circling back to the USS Theodore Roosevelt:
1,156 crew ended up testing positive and had 1 death.
CFR .08%
Matches the CDC estimates for 0-49 pretty well. Like it or not (don't know why anyone would not like it but here we are) the CDC estimates are likely correct for an overall IFR of .26% with the lion's share of that being over 65.
1,156 crew ended up testing positive and had 1 death.
CFR .08%
Matches the CDC estimates for 0-49 pretty well. Like it or not (don't know why anyone would not like it but here we are) the CDC estimates are likely correct for an overall IFR of .26% with the lion's share of that being over 65.
Posted on 5/28/20 at 3:50 pm to buckeye_vol
quote:
1. Point out what is wrong then.
I’m saying that a meta analysis that is fundamentality flawed is no better than a single study.
There are indications that some infections especially in young people and especially asymptomatic cases are being missed by antibody studies.
This post was edited on 5/28/20 at 3:52 pm
Posted on 5/28/20 at 4:16 pm to WaWaWeeWa
quote:Well I found the meta-analysis the CDC used to make their estimates. Let me know if you find this to be flawed:
I’m saying that a meta analysis that is fundamentality flawed is no better than a single study.
1. Published April 6th.
2. 24 studies
3. 21 of them from China
4. The few from outside of China (UK, Germany) have sample sizes below 5 and most are less than 100.
5. The MOST RECENT STUDY was completed in MARCH 5th.
6. Three of of the studies had an IFR OF 0.0% and account for 12% of the Rand effects weighting.
Study used for CDC data
This post was edited on 5/28/20 at 4:17 pm
Posted on 5/28/20 at 4:19 pm to buckeye_vol
Can you link me to where it says that’s all the CDC used to determine IFR
Posted on 5/28/20 at 4:23 pm to WaWaWeeWa
quote:https://www.cdc.gov/coronavirus/2019-ncov/hcp/planning-scenarios-h.pdf
Can you link me to where it says that’s all the CDC used to determine IFR
They cite only 2 sources, and the other one is from 2014 and it’s based on influenza-like illnesses from 2010-2011.
Here are the only 2 sources cited:
quote:
Khalili, M., Karamouzian, M., Nasiri, N., Javadi, S., Mirzazadeh, A., & Sharifi, H. (2020). Epidemiological Characteristics of COVID-19: A Systemic Review and Meta-Analysis. medRxiv.
quote:The first is the one I linked in the previous post, and the lead author is from Iran, which is what the Buzzfeed study is referring to.
Biggerstaff, M., Jhung, M. A., Reed, C., Fry, A. M., Balluz, L., & Finelli, L. (2014). Influenza-like illness, the time to seek healthcare, and influenza antiviral receipt during the 2010–2011 influenza season—United States. The Journal of infectious diseases, 210(4), 535-544.
Although it seemed to find the IFR to be 2% (I saw 0.02 and thought 0.2%) so I’m not sure what the CDC is basing it on now. Of course this is a problem with in and of itself in that it doesn’t provide any documentation, data, or supplemental information to determine how they came to their conclusions.
And note their IFR and R0 estimates contradict one another as the highest IFRs have the highest R0s but a higher IFR would mean there has been less spread per death (i.e., a lower R0).
This post was edited on 5/28/20 at 4:41 pm

Posted on 5/28/20 at 4:39 pm to buckeye_vol
quote:
they didn’t provide what is necessary to make ANY DETERMINATION, especially because the vast majority of studies that have do not support those estimates.
quote:
1. Published April 6th.
2. 24 studies
3. 21 of them from China
4. The few from outside of China (UK, Germany) have sample sizes below 5 and most are less than 100.
5. The MOST RECENT STUDY was completed in MARCH 5th.
6. Three of of the studies had an IFR OF 0.0% and account for 12% of the Rand effects weighting.
Holy shite, that's pathetic. Thanks for digging into it.

 Page 1124 of 1190
Page 1124 of 1190

Popular
Back to top